Enabling smarter prevention through redesign
Enabling smarter prevention through redesign
Cancer screening platform
Cancer screening platform

Client
Client
Lombardy Region / ARIA SpA
Lombardy Region / ARIA SpA
Role
Role
Senior Product Designer
Senior Product Designer
Team lead of two designers in a cross-functional team.
Back-to-back with developers, analysts, product owners and healthcare professionals.
Team lead of two designers in a cross-functional team.
Back-to-back with developers, analysts, product owners and healthcare professionals.
Time span
Time span
January 2025 - July 2025
January 2025 - July 2025
Challenge
Each administrative area, called ATS, managed cancer screening programs using different software systems, based on local processes and governance that were not aligned.
This scenario made it impossible to have a unified overview of the situation, limiting both performance and the ability to compare data against regional targets.
Challenge
Each administrative area managed cancer screening programs using different software systems, based on local processes and governance that were not aligned.
This scenario made it impossible to have a unified overview of the situation, limiting both performance and the ability to compare data against regional targets.
Our goal
Our goal
Build a unified management software meant to align the governance, procedures, and operational expectations of all Lombardy’s local health authorities (ATS).
The project had to ensure regulatory compliance, high reliability, and at the same time show respect and sensitivity for a delicate area like cancer prevention.
Before: a fragmented, inconsistent, & hard-to-use system
Before: a fragmented, inconsistent, & hard-to-use system
What didn't work
What didn't work
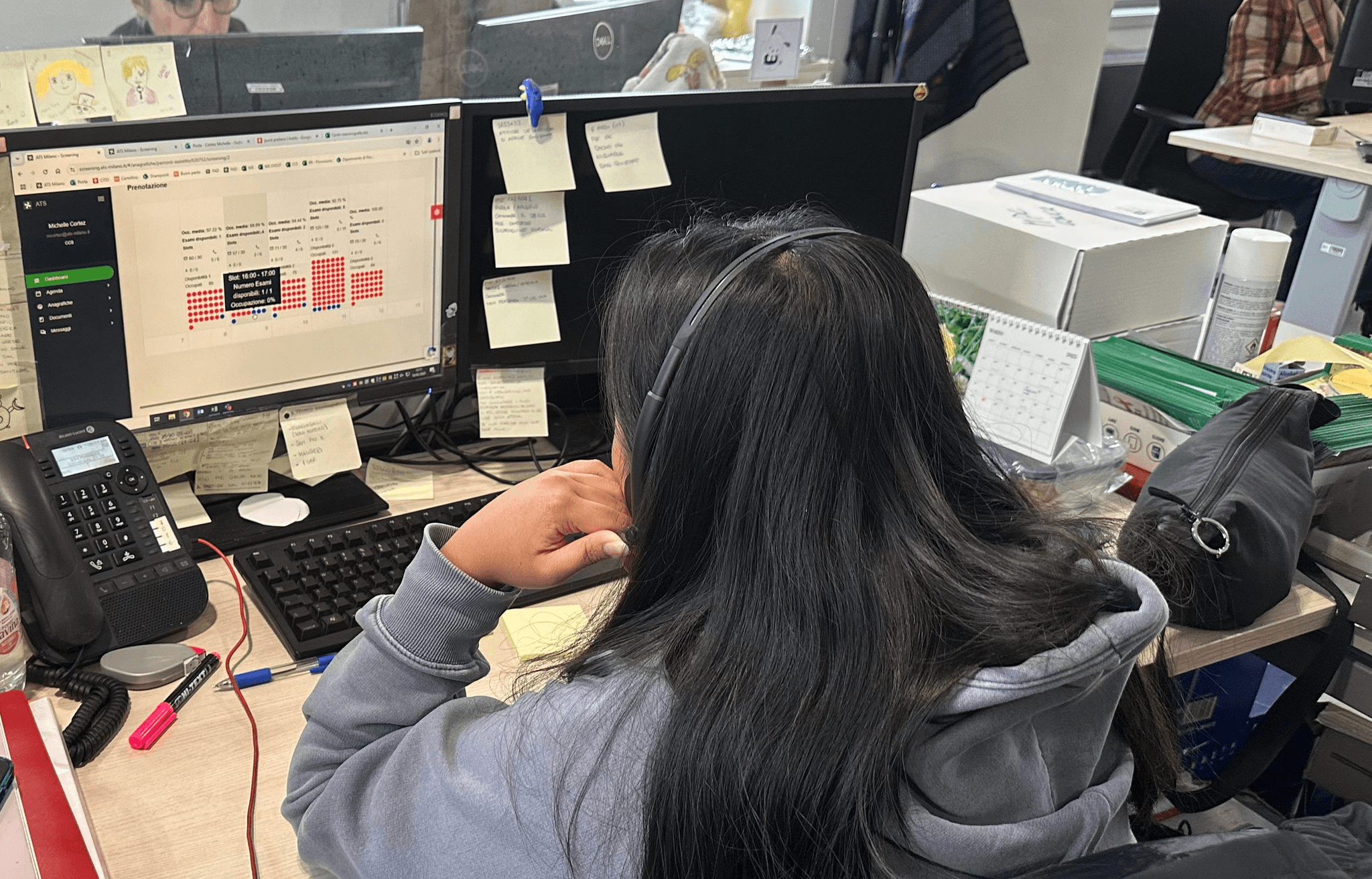
Before the project began, there was a multitude of software tools, processes, and local organizational models. Each ATS operated with different — often customized — systems, making it impossible to compare data at the regional level. Daily operations relied on manual solutions: Excel files, emails, phone calls, increasing the risk of errors and inefficiencies. The result was a system that was unequal, opaque, and difficult to govern.
Before the project began, there was a multitude of software tools, processes, and local organizational models. Each ATS operated with different — often customized — systems, making it impossible to compare data at the regional level. Daily operations relied on manual solutions: Excel files, emails, phone calls, increasing the risk of errors and inefficiencies. The result was a system that was unequal, opaque, and difficult to govern.

Main problems
Main problems
Different systems for each ATS
No shared language,
low comparable data.
Partial and misaligned data
Each software produced different reports — often unusable.
Sensible data shared by private chats
Non compliant, inefficient and clinically risky
Each ATS with its own “rules”
No shared model across territories.
A culture resistant to change
Some staff are wary of digital transformation.
Local Excel files for everything
Used to manage scheduling and follow-ups
Different systems for each ATS
No shared language,
low comparable data.
Partial and misaligned data
Each software produced different reports — often unusable.
Sensible data shared by private chats
Non compliant, inefficient and clinically risky
Each ATS with its own “rules”
No shared model across territories.
A culture resistant to change
Some staff are wary of digital transformation.
Local Excel files for everything
Used to manage scheduling and follow-ups
No cross-ATS mobility
No cross-ATS mobility
"Citizens couldn’t change appointments outside their home ATS."
Such a situation posed a real risk to people’s health. Without a unified, transparent, and coherent system, prevention lost its impact, the Region lost control, and citizens lost trust. It was time to rethink everything, from the ground up.
Such a situation posed a real risk to people’s health. Without a unified, transparent, and coherent system, prevention lost its impact, the Region lost control, and citizens lost trust. It was time to rethink everything, from the ground up.
What I did to keep design aligned, focused and actionable
What I did to keep design aligned, focused and actionable
Strategic activities
Strategic activities
The strategic focus was to align diverse operational models under a unified digital vision, ensuring flexibility for local ATS while enabling centralized orchestration.
The strategic focus was to align diverse operational models under a unified digital vision, ensuring flexibility for local ATS while enabling centralized orchestration.
Shared product vision
Problem space exploration
Comparative analysis
Stakeholder alignment
Prioritization model
Incremental delivery planning
Process governance model
Shared product vision
Problem space exploration
Comparative analysis
Stakeholder alignment
Prioritization model
Incremental delivery planning
Process governance model
Strategic research
Concept sprint (AI-powered)
Feature deep-dives
Strategic research
Concept sprint (AI-powered)
Feature deep-dives
Timeline
Timeline
We balanced systemic vision with targeted accelerations.
The process wasn’t linear, but a coherent progression of strategic pauses, creative leaps, and necessary returns.
We balanced systemic vision with targeted accelerations.
The process wasn’t linear, but a coherent progression of strategic pauses, creative leaps, and necessary returns.
Blueprinting for feature prioritization
Blueprinting for feature prioritization
We approached feature prioritization more like directing a film, rather than making a list.
We approached feature prioritization more like directing a film, rather than making a list.

Psst… Hover to zoom
Psst… Hover to zoom
Building shared vision, navigating complexity
Building shared vision, navigating complexity
Methodology
Methodology
Moderated observations in territorial areas
Happy path workshop
Card sorting workshop
AI prototyping and RITE testing
Monthly focus groups on functional domains
Targeted interviews with screening experts
Usability testing
AI-powered reporting
Development support
We observed healthcare operators at work across different territories, each with its own processes and software.
Output
Mapping of operational differences between ATSs; identification of critical workarounds and recurring systemic inefficiencies.
Moderated observations in territorial areas
We observed healthcare operators at work across different territories, each with its own processes and software.
Output
Mapping of operational differences between ATSs; identification of critical workarounds and recurring systemic inefficiencies.
Happy path workshop
Card sorting workshop
AI prototyping and RITE testing
Monthly focus groups on functional domains
Targeted interviews with screening experts
Usability testing
AI-powered reporting
Development support
Lots of users
Lots of users
We mapped and designed while holding together a wide range of perspectives.
We mapped and designed while holding together a wide range of perspectives.
ATS operator
ATS operator
ATS coordinator
ATS coordinator
Head of ATS
Head of ATS
Hospital operator
Hospital operator
Radiologist
Radiologist
Specialist clinician
Specialist clinician
Laboratory staff
Laboratory staff
Pharmacist
Pharmacist
1.
Even though they all access the same system, users with different operational roles need to land immediately on the tools and information they use most during their daily routine
2.
During calls, operators need instant access to all relevant patient data. If they need to search, switch tabs, or reconstruct information from memory, the flow breaks — and so does the patient’s confidence.
3.
In the absence of a digital list of positive cases, operators organize themselves by manually sharing information files via Microsoft Teams. This informal network fills critical gaps, but it’s fragile, error-prone, and unsustainable at scale.
Key
research
insights
Key
research
insights
Spotlight on the ATS operator journey
Spotlight on the ATS operator journey

"Everything is so much clearer and more convenient than before. I no longer have to guess where to click. The map for choosing a center is a game changer. I can finally find my way at a glance."
"Everything is so much clearer and more convenient than before. I no longer have to guess where to click. The map for choosing a center is a game changer. I can finally find my way at a glance."
Eros, 45, operator at Milan's ATS
Eros, 45, operator at Milan's ATS
Their main activities
Their main activities
ATS operators are the first human point of contact between the screening system and citizens participating in cancer screening programs.
They’re not just “call center agents”: they handle sensitive health data and may build complex calendars. Every action they take contributes directly to prevention.
ATS operators are the first human point of contact between the screening system and citizens participating in cancer screening programs.
They’re not just “call center agents”: they handle sensitive health data and may build complex calendars. Every action they take contributes directly to prevention.
Reschedule appointments in real time while on calls or via email
Call back citizens who tested positive in screenings (e.g. colon)
Call back citizens who tested positive in screenings (e.g. colon)
Usually specialize in a single screening line (e.g. breast, colon, cervical)
Usually specialize in a single screening line (e.g. breast, colon, cervical)

Patient identification
Patient identification
Since ScreenLomb key users have very different needs and work in pressure contexts, we decided to make the homepage different for each user.
For the operator, we decided to set up the homepage as a Google search for patient identification: no mandatory inputs, no scroll.
Since ScreenLomb key users have very different needs and work in pressure contexts, we decided to make the homepage different for each user.
For the operator, we decided to set up the homepage as a Google search for patient identification: no mandatory inputs, no scroll.
Quick search workflow
Quick search workflow
To start a search, operators typically enter the first letter of the name, the first letter of the surname, and the patient’s birthdate. Our system allows them to reach the desired screening line page within just a few clicks.
To start a search, operators typically enter the first letter of the name, the first letter of the surname, and the patient’s birthdate. Our system allows them to reach the desired screening line page within just a few clicks.

Patient page
Patient page
The patient page is an operative dashboard divided into two main sections: the registry part and the screening line part.
Trade-off note:
We were not able to redesign the patient page as extensively as planned, because the section dedicated to reporting the current screening episode was inherited from the application used in Milan. This part relies on a configurator with limited flexibility, leaving little room for further optimization.
The patient page is an operative dashboard divided into two main sections: the registry part and the screening line part.
Trade-off note:
We were not able to redesign the patient page as extensively as planned, because the section dedicated to reporting the current screening episode was inherited from the application used in Milan. This part relies on a configurator with limited flexibility, leaving little room for further optimization.
More than 4 ways to book appointments
More than 4 ways to book appointments
Since this is the first Unified Regional Management System, operators can search for available appointment slots across all ATSs and all facilities — even simultaneously across multiple centers.
To support this new level of flexibility, we designed over four different booking methods, each tailored to specific use cases operators might encounter: Suggested appointments for quick recommendations; Monthly view for broader planning; Daily view for precise slot management; Map view, helpful when searching across different provinces; All-centers mode, ideal for checking availability across multiple locations at once.
Since this is the first Unified Regional Management System, operators can search for available appointment slots across all ATSs and all facilities — even simultaneously across multiple centers.
To support this new level of flexibility, we designed over four different booking methods, each tailored to specific use cases operators might encounter: Suggested appointments for quick recommendations; Monthly view for broader planning; Daily view for precise slot management; Map view, helpful when searching across different provinces; All-centers mode, ideal for checking availability across multiple locations at once.
Move an appointment
Move an appointment
With the Suggested slot feature, operators may reschedule an appointment from the patient page in just 3 clicks.
With the Suggested slot feature, operators may reschedule an appointment from the patient page in just 3 clicks.
Dashboard of positive cases
Dashboard of positive cases
This dashboard addresses the need for a centralized, synchronized space where all operators can access up-to-date information. It enables them to contact patients who tested positive — for example, in cervical screening — and schedule follow-up appointments directly with them.
Another reason why we introduced the list of positive cases was to put an end to the bad practice of sharing sensitive information through informal channels, such as Teams chats.
This dashboard addresses the need for a centralized, synchronized space where all operators can access up-to-date information. It enables them to contact patients who tested positive — for example, in cervical screening — and schedule follow-up appointments directly with them.
Another reason why we introduced the list of positive cases was to put an end to the bad practice of sharing sensitive information through informal channels, such as Teams chats.
Outcomes and next steps
Outcomes and next steps
To validate the effectiveness of the designed experience, we conducted two usability tests with 18 participants representative of the target audience.
To validate the effectiveness of the designed experience, we conducted two usability tests with 18 participants representative of the target audience.
98.6%
98.6%
Average success rate
Average success rate
77.5
77.5
System Usability Scale (SUS) score well above average.
This result aligns with the high task success rate,
reinforcing the impression of a generally positive experience.
System Usability Scale (SUS) score well above average.
This result aligns with the high task success rate,
reinforcing the impression of a generally positive experience.
10/11
10/11
Tasks completed
by 100% of users
Tasks completed by 100% of users
These results show a robust interface.
Only one minor task, about the position and label of a secondary button, showed signs of friction or blocking issues. It was a strong candidate for a focused redesign.
Polishing terminology and affordance transformed the design from very good to effortless.
These results show a robust interface.
Only one minor task, about the position and label of a secondary button, showed signs of friction or blocking issues. It was a strong candidate for a focused redesign.
Polishing terminology and affordance transformed the design from very good to effortless.
More outcomes
More outcomes
Gradual rollout to the rest of the Region
Two more releases already planned
Design of new journeys
for HCV and Lung cancer screening
Extension of features for specialized roles
to other regions and future campaigns
Using AI as a triage system for mammograms
to report autonomously or request human review
Increased alignment
between regional welfare directorate and local health authorities
Gradual rollout to the rest of the Region
Two more releases already planned
Design of new journeys
for HCV and Lung cancer screening
Extension of features for specialized roles
to other regions and future campaigns
Using AI as a triage system for mammograms
to report autonomously or request human review
First rollout planned in ATS Milan
covering 3 screening lines by September 2025
Increased alignment
between regional welfare directorate and local health authorities
What I've
learned from
this project
What I've
learned from
this project
I’ve learned to live with imperfection. Design doesn’t fix everything: sometimes it just creates space for people to work better within real-world constraints.
I’ve learned to live with imperfection. Design doesn’t fix everything: sometimes it just creates space for people to work better within real-world constraints.
You know it’s real public service design when the backoffice stops serving bureaucracy and starts serving people.
You know it’s real public service design when the backoffice stops serving bureaucracy and starts serving people.
The real
success
The real
success
Enabling smarter prevention through redesign
Cancer screening
platform
Client
Lombardy Region / ARIA SpA
Role
Senior Product Designer
Team lead of two designers in a cross-functional team.
Back-to-back with developers, analysts, product owners and healthcare professionals.
Time span
January 2025 - July 2025
Challenge
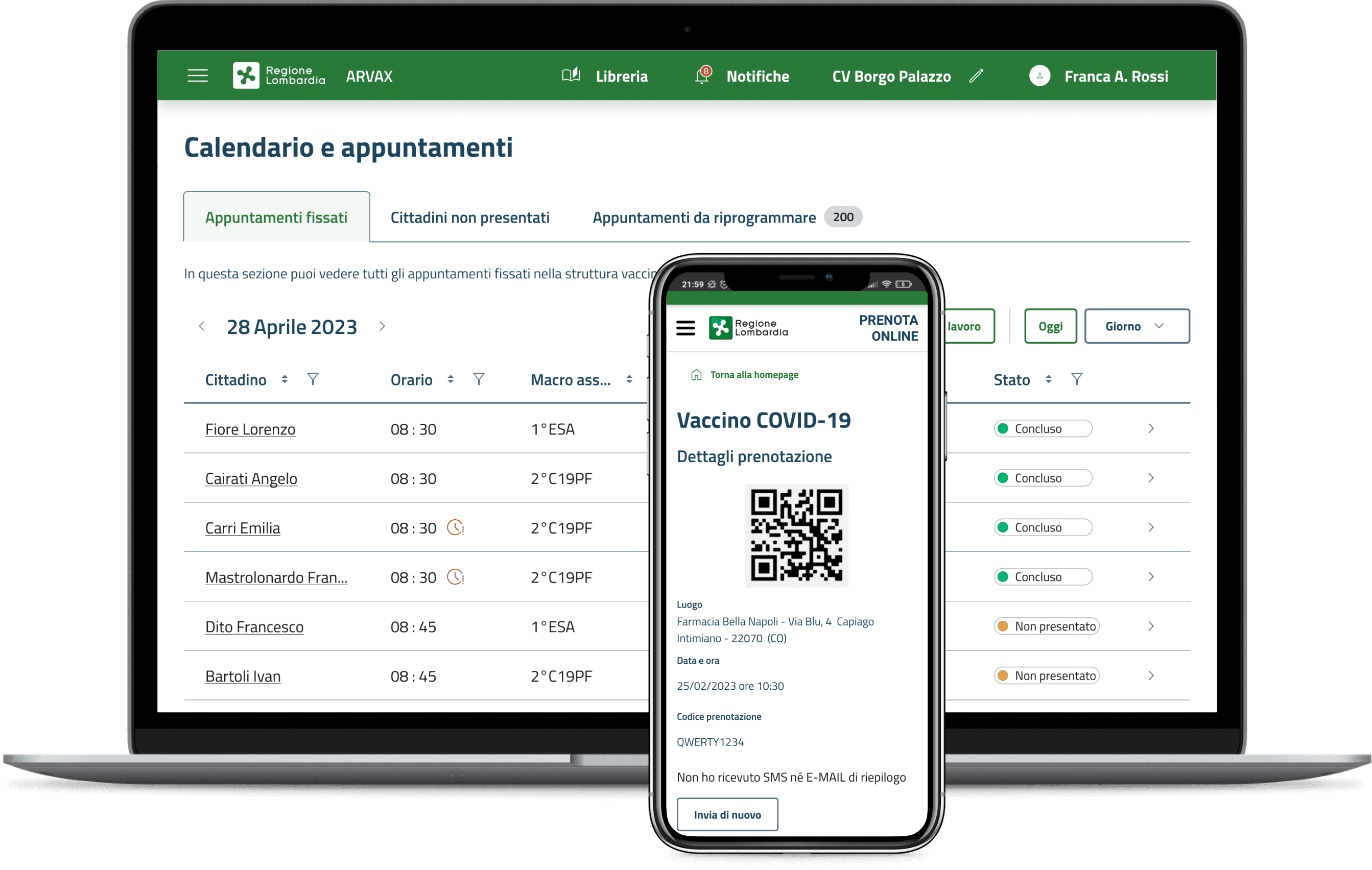
Before our work, vaccination in Lombardy was fragmented across legacy tools, paper forms, and multiple operators with conflicting workflows.
The system lacked agility, coordination, and emergency resilience, especially under
COVID-19.
Our goal
Build a unified management software meant to align the governance, procedures, and operational expectations of all Lombardy’s local health authorities (ATS).
The project had to ensure regulatory compliance, high reliability, and at the same time show respect and sensitivity for a delicate area like cancer prevention.
Before:
a fragmented, inconsistent,
& hard-to-use
system
What didn't work
Before the project began, there was a multitude of software tools, processes, and local organizational models.
Each ATS operated with different — often customized — systems, making it impossible to compare data at the regional level.
Daily operations relied on manual solutions: Excel files, emails, phone calls, increasing the risk of errors and inefficiencies.
The result was a system that was unequal, opaque, and difficult to govern.
Main problems
Partial and misaligned data
Each software produced different reports — often unusable.
Sensible data shared by private chats
Non compliant, inefficient and clinically risky
Each ATS with its own “rules”
No shared model across territories.
Different systems for each ATS
No shared language,
low comparable data.
A culture resistant to change
Some staff are wary of digital transformation.
Local Excel files for everything
Used to manage scheduling and follow-ups
No cross-ATS mobility
"Citizens couldn’t change appointments outside their home ATS."
Such a situation posed a real risk to people’s health. Without a unified, transparent, and coherent system, prevention lost its impact, the Region lost control, and citizens lost trust. It was time to rethink everything, from the ground up.
Strategic activities
The strategic focus was to align diverse operational models under a unified digital vision, ensuring flexibility for local ATS while enabling centralized orchestration.
Shared product vision
Problem space exploration
Comparative analysis
Stakeholder alignment
Prioritization model
Incremental delivery planning
Process governance model
Shared product vision
Problem space exploration
Comparative analysis
Stakeholder alignment
Prioritization model
Incremental delivery planning
Process governance model
Strategic research
Concept sprint (AI-powered)
Feature deep-dives
Strategic research
Concept sprint (AI-powered)
Feature deep-dives
Timeline
We balanced systemic vision with targeted accelerations.
The process wasn’t linear, but a coherent progression of strategic pauses, creative leaps, and necessary returns.
Blueprinting for
feature prioritization
We approached feature prioritization more like directing a film, rather than making a list.

Building shared vision, navigating complexity
What I did to keep design aligned, focused and actionable
Methodology
Moderated observations in territorial areas
We observed healthcare operators at work across different territories, each with its own processes and software.
Output
Mapping of operational differences between ATSs; identification of critical workarounds and recurring systemic inefficiencies.
Happy path workshop
Card sorting workshop
AI prototyping and RITE testing
Monthly focus groups on functional domains
Targeted interviews with screening experts
Usability testing
AI-powered reporting
Development support
Moderated observations in territorial areas
We observed healthcare operators at work across different territories, each with its own processes and software.
Output
Mapping of operational differences between ATSs; identification of critical workarounds and recurring systemic inefficiencies.
Happy path workshop
Card sorting workshop
AI prototyping and RITE testing
Monthly focus groups on functional domains
Targeted interviews with screening experts
Usability testing
AI-powered reporting
Development support
Lots of users
We mapped and designed while holding together a wide range of perspectives.
ATS operator
ATS coordinator
Head of ATS
Hospital operator
Radiologist
Specialist clinician
Laboratory staff
Pharmacist
Key
research
insights
1.
Even though they all access the same system, users with different operational roles need to land immediately on the tools and information they use most during their daily routine
2.
During calls, operators need instant access to all relevant patient data. If they need to search, switch tabs, or reconstruct information from memory, the flow breaks — and so does the patient’s confidence.
3.
In the absence of a digital list of positive cases, operators organize themselves by manually sharing information files via Microsoft Teams. This informal network fills critical gaps, but it’s fragile, error-prone, and unsustainable at scale.
Spotlight on the ATS operator journey
Their main activities
Reschedule appointments
in real time while on calls or via email
Call back citizens who tested positive in screenings (e.g. colon)
Usually specialize in a single screening line (e.g. breast, colon, cervical)
ATS operators are the first human point of contact between the screening system and citizens participating in cancer screening programs.
They’re not just “call center agents”: they handle sensitive health data and may build complex calendars. Every action they take contributes directly to prevention.
Patient identification
Since ScreenLomb key users have very different needs and work in pressure contexts, we decided to make the homepage different for each user.
For the operator, we decided to set up the homepage as a Google search for patient identification: no mandatory inputs, no scroll.
Quick search workflow
To start a search, operators typically enter the first letter of the name, the first letter of the surname, and the patient’s birthdate. Our system allows them to reach the desired screening line page within just a few clicks.
Eros, 45, operator
at Milan's ATS
"Everything is so much clearer and more convenient than before. I no longer have to guess where to click. The map for choosing a center is a game changer. I can finally find my way at a glance."
Patient page
The patient page is an operative dashboard divided into two main sections: the registry part and the screening line part.
Trade-off note:
We were not able to redesign the patient page as extensively as planned, because the section dedicated to reporting the current screening episode was inherited from the application used in Milan. This part relies on a configurator with limited flexibility, leaving little room for further optimization.
More than 4 ways to book appointments
Since this is the first Unified Regional Management System, operators can search for available appointment slots across all ATSs and all facilities — even simultaneously across multiple centers.
To support this new level of flexibility, we designed over four different booking methods, each tailored to specific use cases operators might encounter: Suggested appointments for quick recommendations; Monthly view for broader planning; Daily view for precise slot management; Map view, helpful when searching across different provinces; All-centers mode, ideal for checking availability across multiple locations at once.
Move an appointment
With the Suggested slot feature, operators may reschedule an appointment from the patient page in just 3 clicks.
Dashboard of positive cases
This dashboard addresses the need for a centralized, synchronized space where all operators can access up-to-date information. It enables them to contact patients who tested positive — for example, in cervical screening — and schedule follow-up appointments directly with them.
Another reason why we introduced the list of positive cases was to put an end to the bad practice of sharing sensitive information through informal channels, such as Teams chats.
Outcomes and next steps.

To validate the effectiveness of the designed experience, we conducted two usability tests with 18 participants representative of the target audience.
98.6%
Average success rate
10/11
Tasks completed
by 100% of users
77.5
System Usability Scale (SUS) score well above average.
This result aligns with the high task success rate,
reinforcing the impression of a generally positive experience.
These results show a robust interface.
Only one minor task, about the position and label of a secondary button, showed signs of friction or blocking issues. It was a strong candidate for a focused redesign.
Polishing terminology and affordance transformed the design from very good to effortless.
More outcomes
First rollout planned in ATS Milan
covering 3 screening lines by September 2025
Gradual rollout to the rest of the Region
Two more releases already planned
Design of new journeys
for HCV and Lung cancer screening
Extension of features for specialized roles
to other regions and future campaigns
Using AI as a triage system for mammograms
to report autonomously or request human review
Increased alignment
between regional welfare directorate and local health authorities
The most
valuable
lesson
I’ve learned to live with imperfection. Design doesn’t fix everything: sometimes it just creates space for people to work better within real-world constraints.
The real
success
You know it’s real public service design when the backoffice stops serving bureaucracy and starts serving people.
Want to collaborate? Share an idea?
Or maybe a great recipe?
Contact me
marco.antelmi93@gmail.com
phone
+39 3425084026
©2025
Design & Build by Marco Antelmi
Want to collaborate? Share an idea?
Or maybe a great recipe?
Contact me
marco.antelmi93@gmail.com
phone
+39 3425084026
©2025
Design & Build by Marco Antelmi
Want to collaborate? Share an idea?
Or maybe a great recipe?
Contact me
marco.antelmi93@gmail.com
phone
+39 3425084026
©2025
Design & Build by Marco Antelmi
Marco antelmi
ScreenLomb